Benzodiazepine (BZD) abuse has become a significant public health concern, leading to adverse health outcomes, especially when combined with other central nervous system depressants. The co-abuse of benzos with opioids and alcohol is particularly alarming, contributing to a surge in emergency room visits and fatalities in recent years. While prescription drug abuse, particularly opioid addiction, has garnered considerable attention, benzo addiction remains a less discussed but equally critical issue. Although benzodiazepines are generally considered to have a lower abuse potential in the general population, specific subsets, particularly those with a history of substance use disorders, are at a heightened risk of developing benzo addiction. Education, preventive measures, and early identification are crucial strategies for mitigating benzo addiction.
Introduction to Benzos and Their Addiction Potential
Benzodiazepines were first introduced to the US market in 1960, with chlordiazepoxide being the pioneering drug in this class to gain clinical approval and widespread use.1 Benzos quickly gained favor in medical practice due to their perceived safer profile compared to older sedative medications like barbiturates, primarily because they presented a reduced risk of respiratory depression.1,2
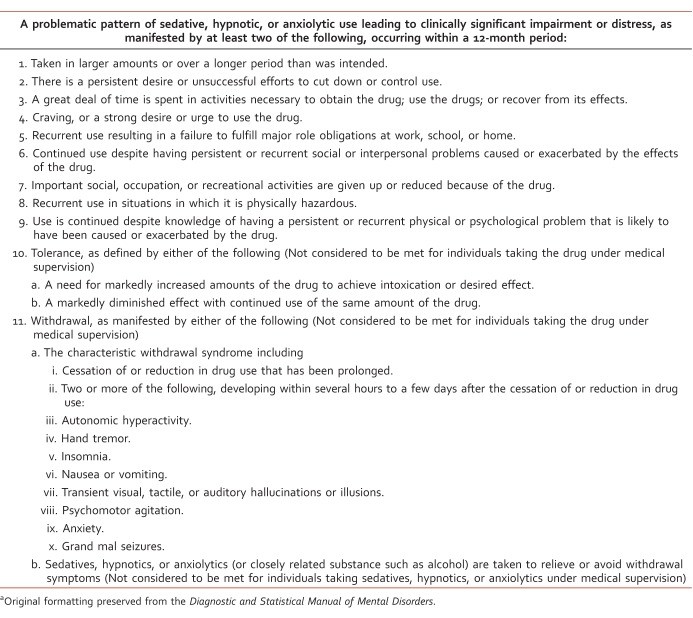
Approximately two decades after their initial discovery, researchers began to elucidate the mechanism of action of benzodiazepines.1 Benzos enhance the effects of gamma-aminobutyric acid (GABA), an inhibitory neurotransmitter, by facilitating its binding to the GABAA receptor. This interaction ultimately leads to an increase in chloride ion flow through ligand-gated chloride channels.3 Concurrently with the discovery of their mechanism, clinicians started to observe instances of benzo abuse and dependence.1 The diagnostic criteria for sedative, hypnotic, or anxiolytic use disorder, which includes benzo addiction, are detailed in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) and summarized in Table 1.4
TABLE 1: Diagnostic criteria for sedative, hypnotic, or anxiolytic use disorder as per DSM-5.
 DSM-5 Diagnostic Criteria for Sedative, Hypnotic, or Anxiolytic Use Disorder
DSM-5 Diagnostic Criteria for Sedative, Hypnotic, or Anxiolytic Use Disorder
Despite the well-established risk of addiction associated with benzos, many aspects remain unclear, particularly concerning the identification of individuals susceptible to benzo addiction and effective treatment strategies for those struggling with benzo abuse. While prescription opioid addiction has received increased research and clinical attention, benzo addiction, despite the availability of safer therapeutic alternatives, continues to be a significant issue as benzos remain among the most frequently prescribed medications.5
Prevalence of Benzos Addiction
In 2008, approximately 75 million prescriptions for benzodiazepines were issued in the United States alone.5 The general population prevalence of benzodiazepine use ranges from 4% to 5%.5,6 Benzodiazepine usage tends to increase with age, and notably, women are prescribed benzos twice as often as men.5,7 Furthermore, individuals who are prescribed opioids are significantly more likely to also receive a benzodiazepine prescription.7,8
While most individuals use benzos as prescribed, it’s estimated that less than 2% escalate to high doses, and an even smaller fraction meet the stringent criteria for benzo abuse or dependence.9,10 In the general population, benzodiazepines are considered to have a relatively low potential for abuse.11 However, certain populations are at a considerably higher risk of benzo addiction, especially those with a personal or family history of substance use disorders.12 Benzo abuse can manifest in two primary patterns: deliberate or recreational abuse aimed at achieving a “high,” and unintentional abuse that originates from legitimate medical use but progresses into inappropriate use over time.13
The misuse and abuse of benzos are increasingly becoming a significant problem. Between 2.3% and 18% of adults in the United States have reported misusing sedatives or tranquilizers, including benzos, for nonmedical purposes at some point in their lives.14–16 Approximately 10% of these individuals develop an addiction, meeting the criteria for abuse or dependence.14 In 2010, there were an estimated 186,000 new cases of benzo abusers.17 Emergency departments have witnessed a dramatic 139% increase in benzo-related visits.18 Advanced age and the presence of other drugs in the system were associated with more severe outcomes, including fatalities.19 Alarmingly, admissions to substance abuse treatment programs for benzo addiction nearly tripled between 1998 and 2008. During this same period, admissions for all substance abuse treatment programs only increased by 11%.20
Risk Factors for Benzos Addiction
Risk factors associated with benzo addiction and the demographic characteristics of this population present some notable differences compared to other substance abuse populations. Firstly, the predominant racial group affected is non-Hispanic White. The role of gender is less clear, as the dominant gender in benzo abuse populations varies across different studies.15,16,20–22 Young adults, particularly those aged 18 to 35 years, constitute the largest proportion of benzo abusers.20,21 Benzo use, misuse, and addiction are strongly linked to co-occurring psychiatric disorders and a personal or family history of substance use disorders.12,15,23,24
Comorbid psychiatric conditions are more prevalent among benzo abusers compared to individuals with other forms of substance abuse.20,21 Approximately 40% of benzo abusers report having a comorbid psychiatric disorder, underscoring the critical need for clinicians to address both the underlying mental health condition and the benzo addiction concurrently.20 Individuals with a history of alcohol abuse or dependence and antisocial personality disorder appear to be at a particularly elevated risk of developing benzo addiction compared to those without either disorder, or those with alcohol abuse or dependence without antisocial personality disorder.22
Benzos Addiction and Polysubstance Abuse
Benzo addiction frequently occurs in combination with the abuse of other substances. For most individuals, benzos are secondary drugs of abuse, with a smaller number reporting benzos as their primary drug of abuse.20 The most commonly reported primary drugs of abuse in conjunction with benzos are opioids (54.2%) and alcohol (24.7%).21 Approximately one in five individuals struggling with alcohol abuse also misuse benzodiazepines.22,25 Benzos are often used to amplify the euphoric effects of other drugs, mitigate undesirable side effects such as insomnia from stimulant use, and manage withdrawal symptoms.2,26,27 Individuals who abuse benzos in combination with other substances tend to consume much higher doses of benzos compared to those who abuse benzos alone.28
In 2010, benzodiazepines were implicated in 408,021 emergency department visits, accounting for one-third of all visits related to pharmaceutical misuse and abuse.18 Specifically, emergency department visits due to the nonmedical use of benzos in combination with opioids saw a significant increase, from 11 per 100,000 population in 2004 to 34.2 per 100,000 in 2011. Benzo involvement in opioid-related fatalities also increased dramatically, from 18% in 2004 to 31% in 2011. Opioids and benzos are the two most frequent classes of prescription drugs involved in overdose deaths.29 Overall death rates related to prescription drug overdoses have surged in recent years.30 Individuals who filled prescriptions for both a benzodiazepine and an opioid faced an almost 15-fold greater risk of drug-related death compared to individuals who were not prescribed either medication.31 Admissions to treatment programs for combined opioid and benzo addiction have skyrocketed, increasing by 570% from 2000 to 2010.21
Opioids are known to cause significant respiratory depression, and this effect is compounded when combined with benzos or alcohol. The interaction between opioids and benzos is complex. Respiration requires activation of excitatory amino acid receptors, while inhibition is mediated through GABA receptors. Respiratory control is centered in the medullary respiratory centers and receives input from peripheral chemoreceptors, which are stimulated by decreases in oxygen and increases in carbon dioxide.32 Benzos, by enhancing GABA activity, reduce respiratory motor amplitude and frequency. Benzos alone rarely cause death.2,12,33,34 While benzos are relatively weak respiratory depressants on their own, they can potentiate significant respiratory depression when used in combination with opioids.32 Opioid actions at the μ opioid receptor lead to reduced sensitivity to changes in oxygen and carbon dioxide levels, causing a decrease in tidal volume and respiratory rate.3,32 Tolerance to opioid-induced respiratory depression develops slowly and incompletely compared to analgesic tolerance.32
Individuals undergoing opioid replacement therapy with methadone or buprenorphine are particularly susceptible to benzo misuse and addiction.35–37 Reasons for the high rates of benzo abuse in this population may include high levels of psychological distress, recreational use, sleep disturbances, attempts to mitigate withdrawal symptoms, reduction of negative effects from other substances like insomnia from amphetamines, and a misperception that benzos are not dangerous drugs.35,36 The lifetime prevalence of benzo abuse was reported as 66.3%, and current abuse as 50.8% in patients receiving methadone replacement therapy.36 More than half of benzo users in methadone maintenance programs did not begin using benzos until after starting methadone treatment.38 Benzo use in combination with methadone is associated with a 60% increase in opioid-related mortality.39 While buprenorphine offers an advantage over methadone due to its ceiling effect, particularly concerning respiratory depression, this ceiling effect diminishes when buprenorphine is combined with benzos.40 Among buprenorphine-experienced individuals, 67% reported concurrent use of benzos, with approximately one-third obtaining benzos from multiple or illicit sources.37
Alcohol is implicated in one in four emergency department visits related to benzo abuse and one in five benzo-related deaths.18 Both alcohol and benzos bind to distinct sites on the GABAA receptor, resulting in synergistic drug actions. Pharmacodynamic interactions, although not fully understood, lead to additive central nervous system depression, reducing the concentrations needed to cause fatal outcomes.41 Benzo-related emergency department visits involving alcohol were most frequent in individuals aged 45 to 54 years, while deaths were more common in those 60 years and older.42 Despite alcohol’s significant role in numerous health conditions, recent data indicate that only one in six adults in the United States report ever discussing their alcohol use with a healthcare professional.43 Prescribers and pharmacists must emphasize patient education regarding the dangers of combining alcohol and benzos. Furthermore, healthcare professionals should implement necessary interventions and referrals when problematic alcohol consumption is suspected or identified.
Abuse Liability and Specific Benzos
Systematic studies comparing the abuse potential among different benzodiazepines are limited. However, pharmacokinetic properties are believed to play a role in abuse liability. Lipophilicity, a chemical property, influences the onset of action.44 Benzodiazepines with higher lipophilicity and shorter half-lives are thought to have a greater potential for abuse.11,13 Chemical properties of commonly prescribed benzodiazepines are summarized in Table 2.44 Evidence from laboratory studies on subjective and reinforcing effects, clinical experience from medical professionals, testimonies from drug abusers, and epidemiological studies collectively suggest that diazepam has the highest abuse liability among benzos.45 Diazepam, alprazolam, and lorazepam received the highest subjective ratings for the “high” they produce in known drug abusers compared to oxazepam, clorazepate, and chlordiazepoxide, which appear to have lower abuse potential.2,11,45,46 In blinded studies, recreational drug users perceived diazepam to be more valuable than equipotent doses of alprazolam and lorazepam.47
Nevertheless, alprazolam and clonazepam are the two benzodiazepines most frequently associated with abuse-related emergency department visits; the rate of alprazolam involvement is more than double that of clonazepam.48 Alprazolam is also the most commonly prescribed benzodiazepine in the United States. Over 44 million alprazolam prescriptions were dispensed in 2009, nearly twice the number of clonazepam prescriptions, which is the second most prescribed benzo in the US. This ease of access may contribute to alprazolam’s higher rate of abuse.49 While pharmacokinetics and user preferences play a significant role in abuse potential, prescribing patterns and the availability of specific agents likely have an equally important influence on benzo addiction rates.50
TABLE 2: Comparative properties of benzodiazepines relevant to abuse potential.
Implications for Healthcare Professionals in Addressing Benzos Addiction
Sources of prescription drug diversion, including benzos, are diverse and can originate from both healthcare-related and non-healthcare-related avenues. The most frequently reported healthcare source of benzo diversion is a regular prescriber, followed by “script doctors” (providers who sell prescriptions), doctor shopping (patients seeking multiple prescriptions from different providers), and pharmacy diversion (e.g., undercounting pills, employee theft).51 Recommendations for identifying high-risk individuals and reducing benzo addiction include: obtaining a detailed personal and family history of substance use, conducting urine drug screens, frequent monitoring for signs of abuse, regularly reassessing the risks and benefits of ongoing benzo therapy, prescribing a limited number of as-needed doses to minimize physiological dependence, and carefully distinguishing between physiological dependence and addiction.12
Patients who engage in “pharmacy shopping,” defined as receiving the same benzo prescription at two different pharmacies within a 7-day period, are at a 5.2 times greater risk of escalating to high doses of benzos compared to other long-term benzo users.9 “Doctor shoppers,” or individuals visiting four or more clinicians within a 6-month period, are more likely to be female and have twice the risk of drug-related death compared to non-shoppers. Pharmacy shoppers, defined as filling controlled substance prescriptions at four or more pharmacies within 6 months, have a 3 times higher risk compared to non-shoppers.31,32 Prescription drug monitoring programs are valuable tools in identifying prescription drug abuse patterns.
Over 90% of unintentional pharmaceutical overdose fatalities exhibit at least one indicator of substance abuse. These indicators include a known history of substance abuse, any instance of drug diversion, nonmedical routes of drug administration, prescriptions from more than five prescribers of controlled substances, contributing alcohol or illicit drug use, previous overdose incidents, and current opioid replacement therapy.33 Both prescribers and pharmacists must be aware of these risks, utilize prescription drug monitoring programs effectively, accurately identify potential drug abusers, and take appropriate steps to mitigate risks. Additional strategies to reduce benzo addiction include limiting the dose, quantity, and number of refills for each prescription.52 Drug diversion is most prevalent among young adults, who typically obtain diverted medications from peers or family members.8,33,52
Past efforts to reduce and restrict benzodiazepine prescribing, such as the implementation of triplicate prescriptions in New York in 1989, had mixed results. While these measures, which included limiting prescriptions to a 30-day supply with no refills for most indications, successfully reduced overall benzodiazepine prescribing, they also had unintended negative consequences.53 These requirements led to a disproportionate reduction in prescribing for low-income and minority populations and also reduced appropriate prescribing. Stringent restrictions inadvertently hindered access to benzos for legitimate medical use.53–56 Healthcare providers and policymakers must exercise caution when implementing laws and strategies to combat prescription drug abuse to avoid impeding appropriate patient care.
Some clinicians argue that the medical community may have overreacted to the risks of benzo addiction, suggesting that this overreaction could lead to underprescribing of a safe and effective class of medications. They advocate for responsible, continued benzodiazepine prescribing when clinically indicated.57 While benzodiazepines do carry a risk of abuse, particularly in populations with substance abuse vulnerabilities, it is crucial to balance these risks with the therapeutic benefits. Prescribers must also consider the risks of untreated illnesses. Poorly managed or untreated anxiety or insomnia can increase the risk of alcohol relapse.58 Evidence-based pharmacotherapy and the use of agents with lower abuse potential should be prioritized as first-line treatments when appropriate. However, benzodiazepines may still be indicated for certain patients at elevated risk of abuse. In such cases, it is essential to provide thorough patient education on the risks of combining benzos with alcohol or other substances, discuss the risks of diversion, prescribe benzodiazepines with lower abuse potential if suitable, closely monitor for adverse effects, and vigilantly monitor for signs of inappropriate use.
Conclusion: Addressing Benzos Addiction Effectively
Prescription drug abuse, including benzo addiction, has reached epidemic proportions. Current efforts to reduce associated morbidity and mortality have not yet been successful, and rates continue to rise. Further research is urgently needed to better understand the risk factors for benzo addiction and develop more effective prevention and treatment strategies. Despite the risks of abuse and diversion, benzodiazepines remain a safe and effective class of medications and continue to play a valuable role in therapy for specific conditions. Policymakers and healthcare professionals face the ongoing challenge of reducing benzo addiction while ensuring accessibility for patients who genuinely need these medications. Efforts should focus on reducing inappropriate prescribing practices rather than broadly restricting all benzodiazepine prescriptions. Education is paramount. Healthcare professionals must stay informed about abuse patterns and diversion trends. It is crucial for prescribers and pharmacists to educate patients not only about the risks to themselves but also the risks to others, to minimize medication sharing and diversion. Identifying benzo addiction risk factors before prescribing, utilizing safer alternatives when possible, and implementing appropriate interventions are critical steps in combating this growing problem. Expanding the availability of substance abuse treatment programs and increasing funding for these programs will be essential in effectively addressing the escalating challenge of benzo addiction.
Footnotes
Disclosures: This material is the result of work supported with resources and the use of facilities at the Fargo Veterans Affairs Health Care System. The contents do not represent the views of the Department of Veterans Affairs or the US government.